


Dr. Robert Malone's explanation of new RSV treatment for infants
This new Vice-Chair of the new ACIP explains in clear language why this new "non-vaccine" makes sense for all infants.


Robert Malone comments regarding the RSV decision
There has been some confusion concerning the nature of the product and the rationale for the decision regarding Enflonsia (clesrovimab). I hope the following will help clarify these issues. Note that this represents a personal opinion, and does not represent the position of the Centers for Disease Control and Prevention (CDC) or the US Government.
Let’s begin by reviewing the key ACIP committee-endorsed language for this product:
ACIP recommends infants aged <8 (less than eight) months born during or entering their first RSV season who are not protected by maternal vaccination receive one dose of Clesrovimab.
Then there was an associated recommendation to add the product to the Vaccines for Children (VFC) program, which (in simple terms) provides federal funding for this and other products to be provided to children and their parents who otherwise could not afford them.
First off, understand that Enflonsia (Clesrovimab) is not a vaccine. It is a second-generation monoclonal antibody preparation that binds to a key protein (fusion or F protein) of the Respiratory Syncytial Virus. It is very similar in efficacy and safety to another product from a different manufacturer already recommended by ACIP for the same indication, that being the product known as Beyfortus (Nirsevimab). These are known as second-generation anti-RSV antibodies, because the first-generation product Synagis (palivizumab), which was licensed by the FDA in 1998. All three of these can help prevent severe RSV illness and death in newborns. Synagis does not last very long after injection, so needs to be injected repeatedly to protect a newborn. The Enflonsia and Beyfortus antibodies have been engineered so that one injection lasts about six months, which is why they are considered second-generation products.
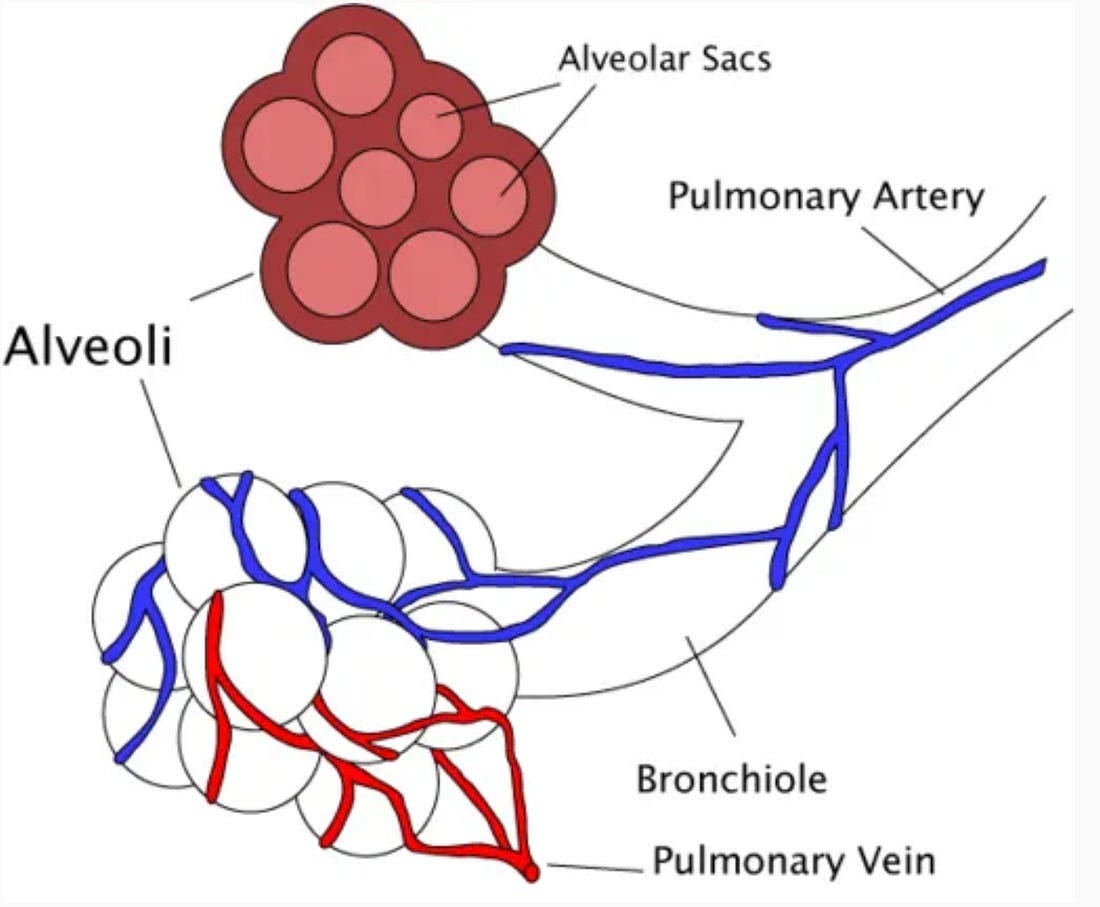
Secondly, why do newborn (and especially premature) children need protection from respiratory syncytial virus? Why just newborns and not all healthy children? After all, virtually every child born in the USA will develop an RSV infection within the first two years of their lives. To understand this requires an understanding of a little bit of lung anatomy. Basically, human lungs use a branching tube to carry air from the outside down to tiny little sacks where the actual gas exchange required for the business of breathing happens. These little sacks are called alveoli. The smallest branches of conducting airway tubes (terminal bronchioles) that take the air to the alveoli are extremely small. In newborns, and especially in premature born infants, these terminal bronchioles are really, really small. So small, that if a newborn gets infected with RSV these tiny tubes swell (due to inflammation) and sort of squeeze closed. And when that happens, the air cannot get down to the alveoli, and it gets really hard for the newborn to get the good air (oxygen) in and the bad air (carbon dioxide) out. So, in a way, they sort of suffocate just like someone was strangling them, only the blockage is way down deep in their lungs.
The good news is that after a year of growth, an infant’s terminal bronchioles grow larger as the young child grows, and it takes a lot more inflammation to squeeze them closed. So if you can get the newborn through the first part of life without RSV causing this problem, then when they do get RSV disease (we all get RSV infections, again and again), the risk of hospitalization or death goes way down. And to be truthful, the risk of hospitalization or death from RSV, even in newborns, is only about 2-3 out of every 100 (2-3%). This may seem like a small number unless your baby is one of the 2-3%. Of that 2-3% (let’s say 3% for discussion), about 20% have identifiable risk factors for severe RSV disease. In other words, they have some problem that makes them more likely to get the illness. 20% of 3% = less than one child out of every 100 births is in the high-risk group that develops severe RSV. The problem is that 80% of those 3% of births that develop severe RSV disease are completely healthy infants. They look just like all of the other healthy newborns - no way to foretell which ones will get really sick with RSV. There is some speculation that these are the same kids who eventually develop asthma in later life, but maybe they develop asthma in later life because they had severe RSV when they were babies. Or maybe we just have not yet figured out what makes them different. But the bottom line is that most of the severe RSV infections - 80%- happen in perfectly healthy newborn children.
Now let’s talk about why the antibody preparations. These are not completely protective but do a pretty good job, and are basically recommended for all newborn children whose mothers were not vaccinated against RSV late in pregnancy.
An aside about vaccination late in pregnancy- virtually all mothers have been previously infected with RSV, so have some degree of natural immunity. Antibody levels gradually drop after recovery from RSV. This is normal- if this did not happen all of us would eventually end up with antibody sludge for blood due to all of our previous infections. If mom decides to accept the RSV vaccine, the product basically acts as a booster to increase their short-term anti-RSV antibody levels. And mom’s antibodies get transferred into baby. So if mom has her level of anti-RSV antibodies boosted up, more RSV antibody ends up in baby. No boosting of mom = less antibodies and more risk to baby if RSV infection happens. Make sense?
Ok, so why do all newborns whose moms did not have their RSV antibody levels boosted need to get this particular jab? For the 20% minority of those who will eventually develop severe RSV disease and have known risk factors, those can be identified before dosing with the product. But here comes the unfortunate reality. If we want to prevent as much RSV hospitalization and death in newborns as possible, the majority of cases occur in newborns with no known risk factors. So, there is no way to sort out beforehand which healthy normal newborns will come down with severe RSV disease. To reduce the risk that the very few healthy newborns who sort of randomly “draw the short straw” end up in the hospital or die, it is recommended that all newborns whose moms did not get their antibodies boosted before delivery receive a dose of one of these long-lasting antibody products before RSV season kicks up.
The members of the current ACIP are very focused on patients, and in this case newborns, and want to minimize any unnecessary injections. We debated at length about this conundrum of dosing all to protect just a small number. But because the majority of the (admittedly rare) severe cases occur in newborns that seem completely healthy at birth, there is just no way to pre-determine which of the healthy ones will get the severe disease. So then it comes down to risk/benefit. And what the clinical data demonstrate is that the risks of the antibody injection are very low, and so are the risks of any one infant developing severe RSV disease. But on balance, the risks of the antibody product injections are much lower than the risk of your otherwise healthy baby being one of the unfortunate few that happens to develop severe RSV disease.
And that is why we voted to recommend this product.
Now why recommend a second product when there is already another one that is recommended? Basically two reasons. First, the supply of the first one might run short some years. And this has happened, so this is not an imaginary risk. The second is that they bind to slightly different places in the RSV F protein. So, if the virus evolves so that one of these products does not work as well, the second one will hopefully still work.
Why is there no significant concern that using these monoclonal products will select for new RSV viruses that are resistant to these antibodies? Because most of the RSV infections are happening in children and adults who are not treated with these products. So this is a very different evolutionary scenario from where everyone is being dosed with a leaky vaccine, such as happened with the SARS-CoV-2 situation.
I hope that the above helps you to understand the decision, to appreciate that the new ACIP team takes these matters very seriously, and that there was robust discussion and examination of all options as well as the risk/benefit considerations before making this recommendation.
I am completely confident that this team will always place the patient (and parents) first when considering recommendations, as was done in this case.
Until next time, best wishes to all concerned, and thank you for following along.